 |
So-called idiopathic scoliosis |  |
| SKOLIOZA / SCOLIOSIS | ABC of scoliosis 1995-2007 |  POLISH VERSION POLISH VERSION |
Partner / książki / books: 
|
Present day explanation of the clinical signs in the biomechanical aetiology of the so-called idiopathic scoliosis (1995 – 2011). The relationship between the “model of hips movement” and the character of scoliosis; three groups and four types. The causative role of “gait” and “standing ‘at ease’ on the right leg” Prof. Tomasz Karski MD, PhD From Vincent Pol University in Lublin E-mail: t.karski@neostrada.pl / tmkarski@gmail.com / www.ortopedia.karski.lublin.pl Keywords Biomechanical aetiology of the so-called idiopathic scoliosis; “syndrome of contractures”, “gait”, “standing” and “model of hip movements”. Abstract The observations from 1985 - 1995 and till 2012 clarify that the development of so-called idiopathic scoliosis is connected with “gait” and habitual permanent “standing at ease” on the right leg. The scoliosis is “a result” of asymmetry of “function” – “changed” loading during gait and asymmetry in time during ‘at ease’ standing, more prevalent on the right leg. Every types of scoliosis is connected with the adequate “model of hips movements” [MHM] (Karski and coll., 2006 [1]). This new classification clarifies the therapeutic approach to each types of scoliosis and provides the possibility to introduce causative prophylaxis.
1. Introduction The “biomechanical influences for development of scoliosis” is presented since 1995 (Congress in Hungary) till now. The aetiology is connected with asymmetry of movements of left and right hips, pelvis and sides left / right of trunk during gait and asymmetry time of “standing at ease” - left leg versus right leg (Karski, 1997). Because of abduction contracture or restricted adduction, the right hip and though that the right leg is “more stronger”, “more stable”, and consequently “more easy for standing”. This asymmetry of movements and asymmetry of function is connected with the “syndrome of contractures” in newborns and babies (Originally in German - “Siebenersyndrom” – Mau [2, 3]).
2. Information about “Syndrome of contractures” As mentioned above the “biomechanical influences in development of scoliosis” are connected with “syndrome of contractures” described by many authors (Hensinger [4], Howorth [5], Green & Griffin [6], Heikkilä E. [7], Tarczynska M., T. Karski, M. Frelek - Karska [8], but in detail by Prof. Hans Mau – Tübingen / Germany - as Siebener [Kontrakturen] Syndrom” (syndrome of seven contractures) [2, 3]. Mostly it is the “left sided syndrome of contractures” as a result of left position of fetus in mother’s uterus 80% - 90% cases (J. Oleszczuk, Lublin [9]). The list of deformities and “asymmetries” are: 1. scull deformity (plagiocephaly, 2. torticollis muscularis (wry neck, 3. infantile scoliosis – other than idiopathic scoliosis, 4. contracture (shortening) of adductor muscles of the left hip 5. contracture (shortening) of abductor muscles and soft tissues of the right hip (Karski [10, 11]), described as Haltungsschwäche (“weak posture”) by Mau. 6. pelvic bone asymmetry – the obliquity of pelvis, 7. foot deformities. In 2006 excessive varus shank deformity (crura vara) was added to the “syndrome of contractures” list, which with the time can lead to Blount disease (T. Karski and coll. [12]).
3. Clinical signs of “syndrome of contractures” in children with so-called idiopathic scoliosis Some authors in the past were able to observe the “symptoms of asymmetry” in different places of child’s body having “idiopathic scoliosis”. The list of authors is as follows: Willner [13], Magoun [14], Wynne-Davies [15], Tylman D. [16], Tarczyńska & Karski & Frelek-Karska [8], Gardner A. [17], Dangerfield P. and coll. [18], McMaster [19], Barlow T. G. [20].
4. Other accompanying deformities, and accompanying illnesses having influence on development of the so-called idiopathic scoliosis These are: (a) joint laxity – makes less stable conjunctions between parts of child’s body, (b) rickets – makes “too plastic bones” which can be more susceptible for deformity, (c) pelvis and lumbar spine anatomy anomalies (spina bifida occulta) – make that spine is less resistant for deformity, (d) the same makes changes in chest and ribs if there are deformed (pectus infundibiliforme) (e) “straight position of trunk (of spine)” in babies and small children with minimal brain deformities or with ADHD can later enables development of scoliosis (Karski [21, 22, 23]).
5. Material. Study of children with so-called idiopathic scoliosis The complete study’s material in 2012 consist of almost 2000 children and adults with scoliosis (N = 1950) from the years 1985 – 2012. The control group (N = 150) – were children examined with “spine problems” – but without any scoliosis.
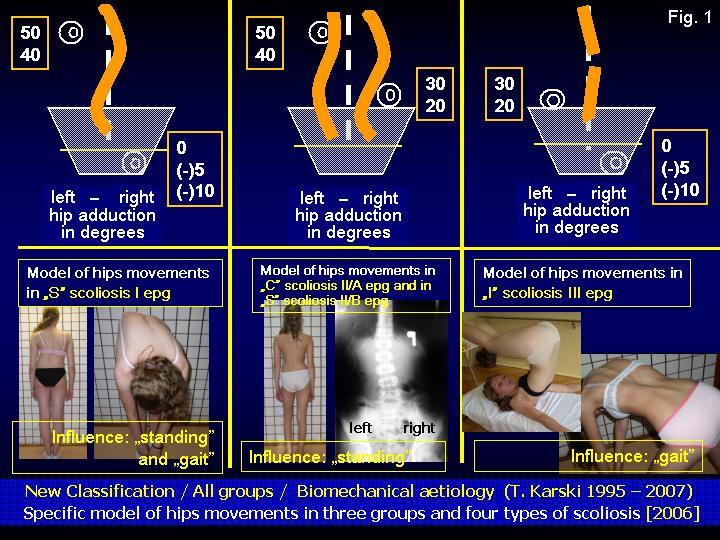
6. New classification. Three etiopathological (epg) groups, four types of scoliosis connected with adequate “model of hips movements
”I-st etiopathological group of scoliosis (“S” - I epg) [Fig. 1] (Karski- observations 1995 - 2012) [“S” deformity = double curve scoliosis]. Cause of deformity: “gait” and “permanent standing on right leg”. The clinical signs in this group are: stiffness of spine with “flat back” because of rotation deformity, as a first signal of scoliosis, but the origin of this deformity lies not in the shoulder (Burwell and coll. [24, 25]) but in the pelvis (Karski [21, 22, 23]). Restricted movements in the right hip (insufficient: adduction, internal rotation and extension) is transmitted “as compensatory movements” on to pelvis and spine and with the time it causes “rotation deformity of spine”. Nevertheless the deformity originating in the shoulder can play an “additional and supportive” role. Similarly - the contracture in the thorax play “supportive role” for progress and fixation of thoracic curve (Sevastik and Diab [26]). Some case in “S” I epg group are “lordoscoliosis”. Both curves arrive at the same time and very early - 2 to 3 years of age. Also presenting early in life is gibbus costalis. This type of scoliosis is progressive especially during the acceleration period of growth.
II-nd etiopathological group of scoliosis – “C” - II/A epg and “S” - II/B epg [Fig. 1] (Karski- observations 1995 - 2012). Cause of deformity: “permanent standing on right leg” for many years. The clinical signs in this group are: “C” left convex curve in lumbar or lumbar – thoracic part of spine, or “S” scoliosis (thoracic deformity second) in children with “laxity of joints” or / and after “harmful exercises”. The first symptoms of this scoliosis present after 10 years of standing.
III-rd etiopathological group of scoliosis [Fig 1] (Karski- observations 1995 - 2012). Karski. The spine deformation in this group is with little or no curvature”. Cause of deformity: “gait” but not “standing” because the stability of hips - left / right - during standing is similar and therefore no “predominance of standing on the right leg” is evident. The main symptom in this group is “stiffness of spine”. In this group clinically and radio-graphically we see no curves, or only slight deformities. We also see little or no rib hump.
7. New tests for scoliosis – short information [21] In the diagnosis of scoliosis we should use known examinations techniques (Adams & Meyer test [27, 28]), as well as new tests such as “side bending test for scoliosis”, checking for the habit of standing (right versus left leg), the Elly-Dunkan [21] test (or Thom test or Staheli test), pelvis rotation test (new test – 2006), “adduction of hips test – similar to Ober test” [21] and others.
8. New rehabilitations exercises – short information [21] All extension exercises and “strengthening exercises” recommended in the past have been wrong and incorrect. New exercises were introduced in the years 1985 – 1995 and have been performed in our Department. These are exercises that remove contractures in the region of the hips, pelvis and spine. There are also flexion- rotation exercises for the spine and these have proven to be very effective for all endangered children, especially those in early childhood; 3-rd or 4- th years. Over the years we have also made numerous observations and confirmations that the solution for “spine problems” is only prophylactics, based on the “biomechanical aetiology of scoliosis”.
9. Conclusions 1. The aetiology of so-called idiopathic scoliosis is strictly biomechanical and the explanation is based on asymmetrical movements of the hips during gait and asymmetry of standing on legs – more on the right leg. 2. The groups of scoliosis in new classification (2001 – 2004 / 2006) are determined in connection with “model of hips movements” (Karski, 2006). 3. There are three group and four types of scoliosis: “S” - I epg, “C” - II/A epg – “S” - II/B epg and “I” – III epg. 4. All at-risk children should be included in an early program of “prophylactics” using stretching exercises. Active sports like: karate, kung fu, taekwoon do, tai chi, aikido, yoga etc. are also very beneficial.
References [1] Karski T., Kalakucki J., Karski J. „Syndrome of contractures” (according to Mau) with the abduction contracture of the right hip as causative factor for development of the so-called idiopathic scoliosis” in Technology and informatics, vol. 123, Research into spinal deformities, 5 Ed. D. Uyttendaele, P. H. Dangerfield, p. 34 – 39, Washington 2006, IOS Press [2] Mau H. Zur Ätiopathogenese von Skoliose, Hüftdysplasie und Schiefhals im Säuglinsalter. Zeitschrift f. Orthop.1979, 5,601-5. [3] Mau H. Die Atiopatogenese der Skoliose, Bücherei des Orthopäden, Band 33, Enke Verlag Stuttgart 1982, 1 - 110 [4] Hensinger RN. Congenital dislocation of the hip. Clinical Symp. 1979, 31 [5] Howorth B. The etiology of the congenital dislocation of the hip, Clin. Orthop., 1977, 29, 164-179 [6] Green NE, Griffin PP. Hip dysplasia associated with abduction contracture of the contralateral hip. J.B.J.S.1982, 63-A,1273-1281. [7] Heikkilä E. Congenital dislocation of the hip in Finland. An epidemiologic analysis of 1035 cases, Acta Orthop. Scandinavica 1984, B.55,125-129. [8] Tarczyńska M, Karski T, Frelek-Karska M. Prenatal conditions for the development of the hip dysplasia in the material of 223 pregnant women, followed-up study of the newborn children”. EPOS 2000, XIX Meeting of the European Pediatric Orthopaedic Society, Congress Book, Milan, April 5-8.2000, page P8. [9] Oleszczuk J., Szymański W., Wilczyński: "Patologia ciąży" in 'Położnictwo" Klimek Rudolf, Dream Publ. Comp.Inc.,Kraków, 1999, pp. 395 - 499 [10] Karski T. Hip abductor contracture as a biomechanical factor in the development of the so-called „idiopathic scoliosis”. Explanation of the etiology, Magyar Traumatologia, Ortopedia, Kezsebeszet, Plasztikai Sebeszet, 1998, 3, 239 - 246 [11] Karski T, Karski J, Madej J, Latalski M. Persönliche Überlegungen zur Ätiologie der idiopathischen Skoliosen. Praktische Hinweise zur Entdeckung beginnender Skoliosen. Prinzipien der neuen Übungstherapie. Möglichkeiten der Prophylaxe. Orthop. Praxis, 02/2002, 38, 75 – 83 [12] T. Karski, Z. Drabik, J. Karski, E. Agbemey Osteotomien in der Behandlung von Kindern mit Crura vara ( M. Blount ), Orthop. Praxis, Heft 9, September 1994, 582 – 585 [13] Willner (1972) in Normelly H.: Asymmetric rib growth as an aetiological factor in idiopathic scoliosis in adolescent girls, Stockholm 1985,1-103. [14] Magoun (1974) in Normelly H. Asymmetric rib growth as an aetiological factor in idiopathic scoliosis in adolescent girls, Stockholm 1985,1-103. [15] Wynne-Davies (1975) in Normelly H: Asymmetric rib growth as an aetiological factor in idiopathic scoliosis in adolescent girls, Stockholm 1985,1-103. [16] Tylman D. Patomechanika bocznych skrzywień kręgosłupa, Wydawnictwo Severus, Warszawa, 1995, Pages 167. [17] Gardner A. in Karski T. Skoliozy tzw. idiopatyczne – przyczyny, rozwój i utrwalanie się wady. Profilaktyka i zasady nowej rehabilitacji. The etiology of the so-called idiopathic scoliosis. Progress and fixation of the spine disorders. The prophylaxis and principles of the new rehabilitation treatment, KGM, Lublin, 2000, 1 – 143 [18] Dangerfield PH, Dorgan JC, Scutt D, Gikas G, Taylor JF. Stature in Adolescent Idiopathic Scoliosis (AIS).14 Meeting EPOS, Brussels, 5-April 1995, Papers and Abstracts, Page 210. [19] McMaster MJ. Infantile idiopathic scoliosis: can it be prevented?” J. B. J. S., 1983, 65-B, 612-617 [20] Barlow TG. Early diagnosis and treatment of congenital dislocation of the hip. J.B.J.S., 962, 44B(2), 292-301 [21] Karski T. Etiology of the so-called “idiopathic scoliosis”. Biomechanical explanation of spine deformity. Two groups of development of scoliosis. New rehabilitation treatment. Possibility of prophylactics, Studies in Technology and Informatics, Research into Spinal Deformities 4, Vol. 91., IOS Press 2002, Amsterdam, Berlin, Oxford, Tokyo, Washington DC, 37-46. [22] Karski T. “Skoliozy tzw. idiopatyczne- etiologia, rozpoznawanie zagrożeń. Nowa klasyfikacja (2001 – 2004/2006). Nowe leczenie rehabilitacyjne. Profilaktyka. The etiology of the so-called idiopathic scoliosis. New classification (2—1 –2004/2006). The new rehabilitation treatment. Prophylaxis. Ätiologie der sogenannten idiopathischen Skoliosen. Drei pathogenethische Gruppen, vier Typen der Wirbelsäuledeformitäten. Neu Übungstherapie. Prophylaxe“. Drukarnia KGM, Lublin, 2011, stron 420 [23] Karski T. Biomechanical Explanation of Etiology of the So-Called Idiopathic Scoliosis. Two etiopahtological Groups - Important for Treatment and Neo-Prophylaxis Pan Arab Journal Vol. (9) No. (1)/ January 2005 pp 123-135 [24] Burwell RG, RK Aujla, AS Kirby, PH Dangerfield, A. Moulton, BJC Freeman, AA Cole, , FJ Polak, RK Pratt, JK Webb “Leg – arms length ration correlate with severity of apical vertebral rotation in girls after school screening for adolescent idiopathic scoliosis (AIS): a dynamic pathomechanism in the initiation of the deformity?” Technology and Informatics, Research into Spinal Deformities 6, Editor: Peter H. Dangerfield, IOS Press, Amsterdam-Berlin-Oxford-Tokyo-Washington, 2008, 189 - 193 [25] Burwell G, Dangerfield PH, Lowe T, Margulies J. Spine. Etiology of Adolescent Idiopathic Scoliosis: Current Trends and Relevance to New Treatment Approaches, Volume 14/Number 2, Hanley&Belfus, Inc, May 2000., Philadelphia, str 324 [26] Sevastik J, Diab K. Studies in Technology and Informatics, Research into Spinal Deformities 1, Vol. 37., IOS Press 1997, Amsterdam, Berlin, Oxford, Tokyo, Washington, DC 1-509. [27] Adams in Tomaschewski R, Popp B. Die Funktionelle Behandlung der beginnenden idiopathischen Skoliose. Jahann Ambrosius Barth, Leipzig Heidelberg 1992, 1-96. [28] Meyer in Tomaschewski R, Popp B. Die Funktionelle Behandlung der beginnenden idiopathischen Skoliose. Jahann Ambrosius Barth, Leipzig Heidelberg 1992, 1-96. Fig. 1 Three group and four types of scoliosis connected with “model of hips movements”. Causative influence: for “S” scoliosis I epg – “gait” and “standing on right leg”, for “C” II/A epg and “S” II/B epg scoliosis – “standing on right leg”, for “I” III epg scoliosis – “gait” only. Address: 20-825 Lublin, Urocza Street 19 Phone: 0048/81/7426371 tmkarski@gmail.com t.karski@neostrada.pl |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||





| Data modyfikacji: 2012-10-14 | Strona przygotowana przez Prof. dr med. Tomasza Karskiego | |||
 |
 |